Case 1: Question
18 year old male presented for initiation of MDI Regimen. His weight in 80kg. He is not confident carb counting yet.
Intro to Insulin Dosing
Total Daily Dose (TDD)
Total Daily Dose (TDD) of insulin is weight based and calculated from patient’s weight in kilograms. TDD=Factor x weight in kilograms. Factor of 0.3-0.5 is used as a starting point for initial insulin regimens. Higher insulin resistance will result in higher insulin requirements and higher factor.
The Total Daily Dose is then split 50/50 (or 40/60 in newer formulas for T1DM) into basal and bolus insulin respectively.
Basal Insulin (TBD)
Basal insulin works continuously to match the continuous output of glucose from the liver produced by gluconeogenesis. Basal insulin can be supplied as a basal rate in U/hr by Continuous Subcutaneous Insulin Infusion (CSII) i.e. insulin pump, or by subcutaneous injection of insulin analogs with long half lives.
Bolus Insulin
Bolus insulin is given in multiple injections either to cover glucose intake from food or to correct for an elevated blood glucose. Bolus insulin can be delivered by administration of insulin analogs with very short half lives via subcutaneous injection, by inhalation, or by bolus delivery from CSII device.
Mealtime bolus insulin can be given in a fixed dose regimen where it is split evenly between three meals. Otherwise, for patients who are comfortable counting carbs, bolus insulin can be matched to carb intake by using a Carbohydrate to Insulin Ratio (CIR) which specifies that number of grams of carbs covered by 1U of insulin. CIR can be calculated as follows: CIR=450/TDD
Correction bolus insulin is typically as an addition to mealtime insulin if glusoe is above goal during a premeal check. The additional correction insulin is based on a Correction Facotr (CF), otherwise known as an Insulin Sensitivity Factor (ISF) and can be calculated from the total daily dose of insulin as follows: CF=1700/TDD
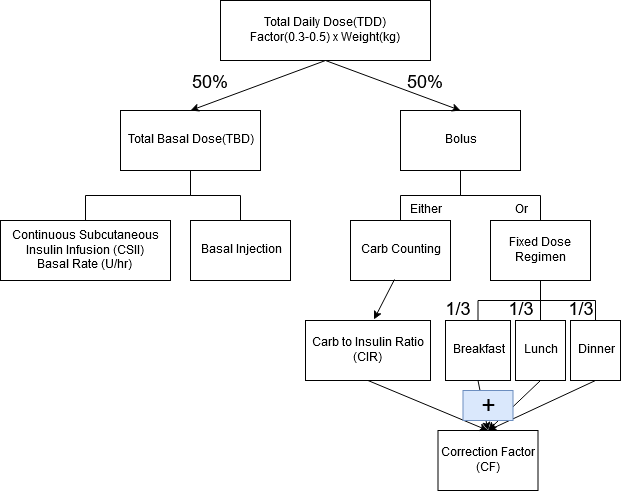
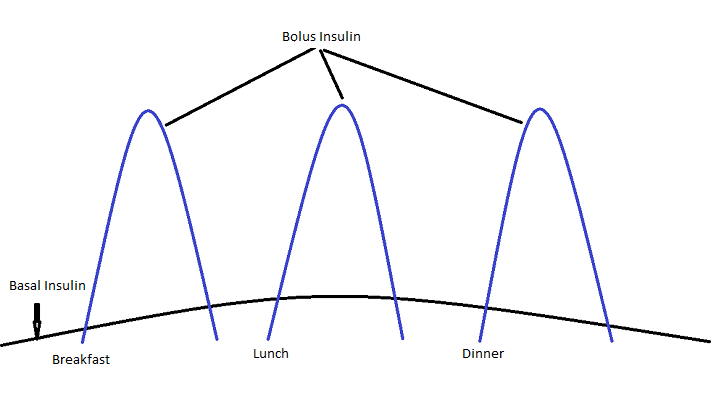
Figure 3. Insulin types and pharmacokinetics. Typically use rapid and short insulin for bolus, long and intermediate for basal.
ADA and AACE have good practice guidelines for insulin dosing.
Insulin Regimen Calculator
Insulin regimen calculators can make it simple to calculate insulin regimens for patients. This calculator uses formulas from AACE guidelines: TDD=factor x weight, CF=1700/TDD, CIR=450/TDD, TBD=0.5*TDD. Dosing based on factor between 0.3 and 0.5 can be considered for starting regimens for DM. In our case, 0.4 was used. A more sophisticated calculator can be found at https://insulin.ddns.net
Try calculating regimens for other patients
Other formulas
1700 rule, 1500 rule, 500 rule…
There are many other formulas proposed for insulin dosing. They are, for the most part, derived from studies of Continuous Subcutaneous Insulin Infusion (CSII) utlizing regression analysis to synthesize formulas that are easy to use in clincal practice. The following is a good review article on various dosing formulas: https://www.ncbi.nlm.nih.gov/pubmed/27457238
Below, you can see a comparison of dosing paramaters derived from the different formulas.
Key:
- AACE guidelines: CF=1700/TDD, CIR=450/TDD, TDD=factor x weight, TBD=0.5*TDD
- King 2016: CF=1700/TDD, CIR=400/TDD, TDD=factor x weight, TBD=0.4*TDD
- Prospective Study, King 2010: CF=1500/TDD, CIR=300/TDD, TDD=factor x weight, TBD=0.4*TDD
- Retrospective Study, Walsh 2010: CF=1960/TDD, CIR=[2.6*Wt(lbs)]/TDD, TBD=0.476xTDD
- Retrospective Study, Davidson 2008: CF=1694/TDD, CIR=441/TDD, TBD=0.47*TDD
- Retrospective Study, Davidson 2003: CF=1724/TDD, CIR=[2.8*Wt(lbs)]/TDD, TBD=0.48*TDD. Statistically based CSII prameters Diabetes Technol Ther. 2003;5:237
1 Month Followup
The patient brings blood glucose log to his 1 month followup appointment. Results are as follows:
How would you change his regimen?
Old regimen was: Basal: 16U, Bolus: 5U TIDAC, CF 53
Calculator to increase regimens
Device trend data
Many glucose monitoring devices provide trends to assist with quickly analyzing glucose logs. This makes it easier to spot trends and outliers more efficiently. The following plots utilize the same 1 month followup data as in the previous question
It is clear from these plots that BG is above goal at every check with no episodes of hypoglycemia.
A tool to allow an in depth analysis of any blood glucose log uploaded in excel format can be found at https://insulin.ddns.net
Glycemic goals
There are several different guidelines for glycemic goals for DM. Newer guidelines emphasize individualizing glycemic targets based on individual patient characteristics. The following is a summary of ADA guidelines for DM based on health status and age category:
For more information and definitions, see ADA guidelines:
SMBG
The initial insulin regimen is an educated guess that is based on:
- Weight of Patient (kg)
- Formulas from prospective and retrospective studies
After the initial regimen is initiated, the patient is instructed in Self Monitoring of Blood Glucose (SMBG). There are four primary times to check:
- Fasting Blood Glucose (FBG). This is usually before breakfast
- Pre-Lunch
- Pre-Dinner
- Bedtime
These checks help to inform adjustments of basal and prandial insulin (Figure 3).
- FBG informs basal insulin adjustment
- Pre Lunch informs breakfast prandial insulin adjustment
- Pre Dinner informs lunch prandial insulin adjustment
- Bedtime informs dinner prandial insulin adjustment
For example, if BG increases significantly between pre lunch and pre dinner checks, lunch prandial insulin may need to be adjusted
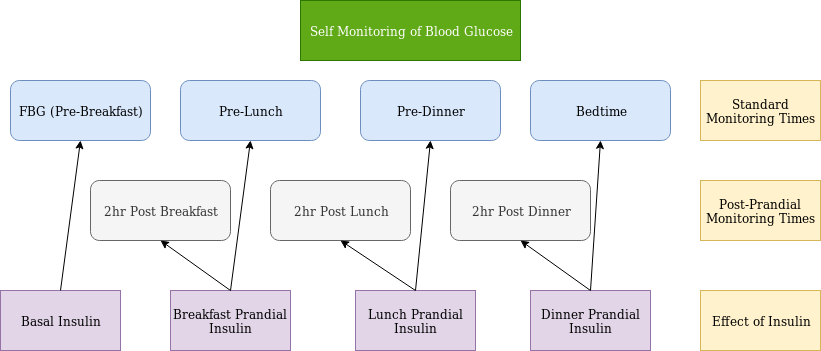
If pre-prandial checks are at goal, but A1c is still elevated, guidelines recommend post-prandial checks as post-prandial excursions may be responsible for persistently elevated A1c despite goal pre-prandial checks.
Examples:
Example 1
Example 2
Example 3
Predict A1c from average glucose
At his initial one month appointment, the patient asks what his predicted A1c would be as it is too early to repeat an serum HgbA1c. Luckily, many BG monitoring devlices provide summary information. Also, a tool is available at https://insulin.ddns.net that will provide this information for any BG log uploaded in excel format. His BG monitoring device provided the following summary information.
Predicted A1c calculator
There are several calculators available online to assist with predicting A1c. One is available at https://insulin.ddns.net. A simple table can also help with general knowledge of A1c/eAG relationship.
A1c Table
3 Month followup
Patient presents to his 3 month followup. Log data follows. He has learned carb counting since the last visit and would like to be switched to a carb ratio regimen.
What would you recommend for his new regimen?
Old regimen was: Basal: 18U, Bolus: 6U TIDAC, CF 46
6 Month followup
Patient presented for 6 month followup. Blood sugar log data follows:
Carb Counting Basics
Determining and adjusting CIR
The initial CIR can be calculated by CIR=450/TDD. Signs that the CIR may need to be adusted
- Large post prandial excursions
- BG dropping or significantly increasing between pre-prandial checks
- Fasting and premeal checks within goal, but elevated HgbA1c. (May have uncontrolled postprandial BG)
CIR can be tested via test meal.
Test meal
Patient eats a test meal of known carb content and less than 20g of fat when BG is in range [70-140]. BG is then checked 2 hours later with expected increase in BG 30-50. If BG increases less than 30mg/dL, then CIR is too low. If BG increases more than 50mg/dL, then CIR is too high.
How to carb count
Calculating the amount of carbs in grams is essential to properly dosing insulin if using CIR. A simple mistake such as not reading serving sizes correctly, could result in significant errors in insulin dosing. For this reason, a carb counting regimen is only used for patients who are very comfortable counting carbs and a fixed dose regimen is usually the initial dosing regimen.
There are many tools to assist with carb counting. Many of these tools utilize the same FDA food database which can be accessed at:
How to calculate how much insulin to give for a meal
Calculating the amount of insulin for a meal is fairly simple utilizing Carb to Insulin Ration (CIR). CIR is the amount of carbs that 1 U of insulin will cover.
9 Month followup
The patient comes to his 9 month followup. He stated that he has been doing much better with carb counting. BG log data follows:
Day 27
You see that day 27 had particluarly high numbers and ask the patient what happened that day. You can focus on day 27 by hovering over it in the scatter plot or going to page 3 on the table. He stated that he forgot to take his morning insulin on that day. He took his lunch and dinner insulin as well as correction insulin throughout the day; however, the blood glucose never came down. He has noted that whenever he has had high blood glucose in the past, he has not been able to successfully bring it down with correction insulin.
Correction Insulin
The patient asks for an example of how to use his new correction factor (38).
Correction Factor vs Correction Scale vs Sliding scale
There are three main ways to give correction insulin.
- Calculating it using the correction factor and a goal glucose
- Using a correction scale based on correction factor and goal glucose
- Using sliding scale (least flexible way)
1. Correction factor and goal glucose
The formula ‘units of insulin=(current BG-Goal BG)/CF’ can be used to calculate a correction dose utilizing CF, goal glucose, and current glucose. There are numerous calculators on the internet to assist with this calculation, one is available at https://insulin.ddns.net. This is the preferred method when using an insulin pump where very small increments of insulin can be delivered precisely and where the calculation is done automatically by the pumps ‘bolus wizard’. You can try some calculations below.
2. Correction scale based on correction factor and goal glucose
In patients who do not have a pump (so can only deliver insulin in increments of 1U), the precision of the previous formula is not necessary and the calculation can be difficult for some patients when they don’t have the convenience of a ‘bolus wizard’ in a pump. In such cases, a correction scale based on the CF, goal glucose, current glucose which uses increments of 1U may be preferrable. A tool to automatically make this scale is available at https://insulin.ddns.net and can be exported in a variety of ways (print, pdf, excel). An example of this type of correction scale is provided below:
3. Sliding Scale
Sliding Scale Insulin is a much older method of delivering correction insulin and is still widely used due to its convenience and simplicity. It uses increments of 50mg/dL blood glucose instead of the custom increments of the previous corrrection scale. However, this means that it is not as versatile as the previous methods, and when a custom correction scale is so simple to make and export using a webapp such as https://insulin.ddns.net, the added simplicity of a sliding scale is not usually needed. Below is an example of a sliding scale and how it can be made and customized.
12 Month Followup
The patient returns for his 12 month followup visit. SMBG data are shown below.
His current regimen is: Basal: 18U, Bolus: CIR 12, CF 38
BOB
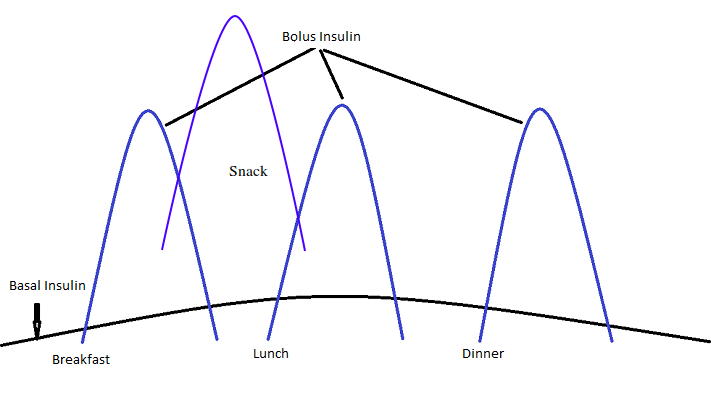
Insulin Stacking
Duration of bolus insulin analogs (lispro, aspart) is approximately 3-5 hours. Therefore, delivering this insulin any more frequently will result in stacking of insulin if the amount of active insulin (Bolus on Board) is not taken into account in the bolus calculation. This is what was occuring with the patient between breakfast and lunch. He was bolusing for a snack two hours after bolusing for breakfast without taking into account the active insulin that was still present from breakfast. This is illustrated in Figure 4.
Bolus on Board (BOB)
The bolus on board, or insulin on board, represents the continued action of an insulin bolus that was given previously. It is derived by the Duration of Insulin Action (DIA), otherwise known as the Active Insulin Time (AIT). The usual starting DIA is 4 hours, but can frequently range between 3-5 hours which is the usual duration of insulin analogs lispro and aspart. CSII devices automatically keep track of boluses and factor in BOB when calculating boluses in the “bolus wizard”. For patients not using CSII devices, BOB can be estimated with the following equation: BOB=PriorBolus-[PriorBolus X (\(\frac{Time Since Last Bolus}{DurationofInsulinAction}\))]. The BOB is subtracted from the bolus that would have been given based on carbs and correction to produce a lower amount of insulin that takes into account the action of bolus insulin given previously. However, as one can surmise from the equation, if the time since the last bolus is \(\ge\) the DIA, the BOB calculation does not need to be done as the prior insulin bolus no longer has any action.
Putting it all together. Complete bolus calculations.
The BOB equation can be combined with the correction equation and the CIR equation to give a final determination of the bolus that should be given taking into account the active insulin from prior boluses. It is important to take into account BOB if an insulin bolus has been given recently e.g. more recently than the DIA. In a practical sense, this is important mainly when considering boluses for snacks between meals.
Complete bolus equation: [Insulin for correction + Insulin for Carbs] - Bolus on Board
[\(\frac{Current Glucose-GoalGlucose}{Correction Factor}\)+\(\frac{Grams Of Carbs}{CarbtoInsulinRatio}\)]–[PriorBolus-(PriorBolus X \(\frac{Time Since Last Bolus}{DurationofInsulinAction}\))]
This can be a difficult calculation to do for every bolus. There is a calculator available to assist with this calculation at https://insulin.ddns.net A sample calculator is provided below.